Asbestosis is the general term for a group of naturally occurring fibers composed of hydrated magnesium silicates.
The spectrum of pleuropulmonary disorders associated with asbestos exposure includes:
Asbestosis;
Pleural disease; and
Malignancies.
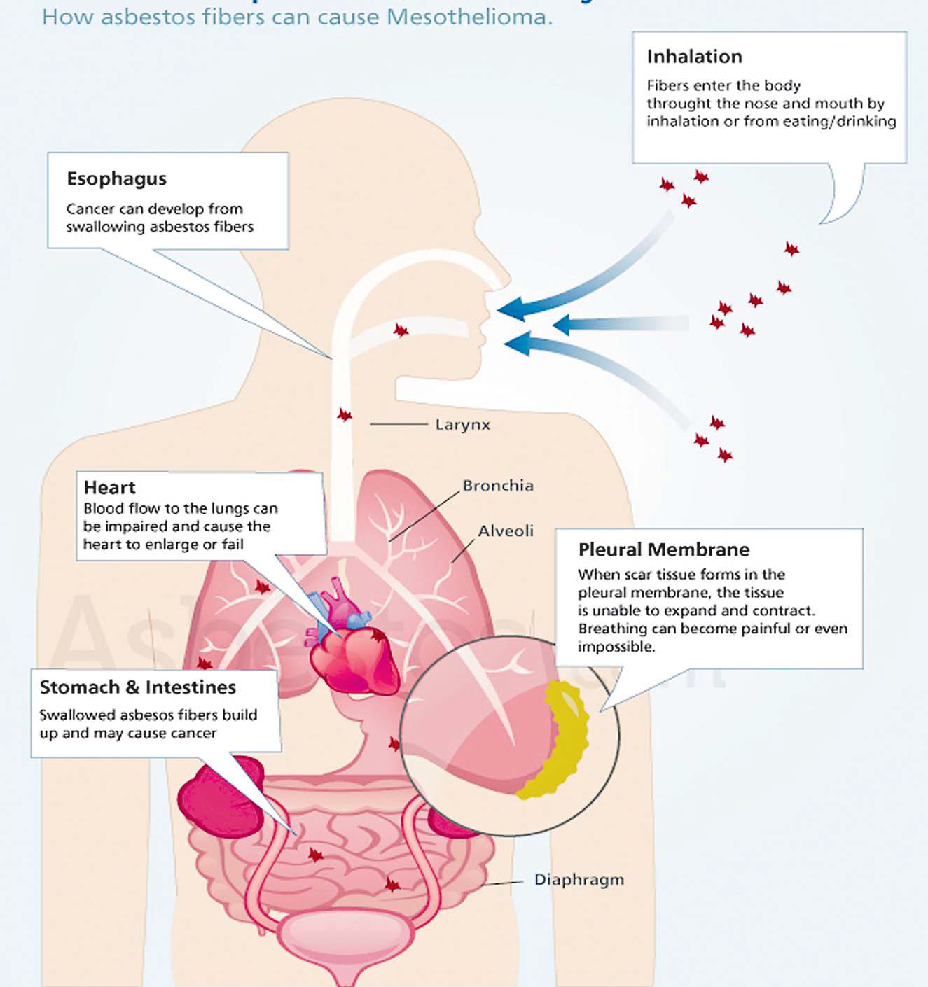
Asbestosis specifically refers to the pneumoconiosis caused by inhalation of asbestos fibers. (Fibers are divided into two categories based on their shape which are: Serpentine and amphibole fibers. The disease is characterized by slowly progressive, diffuse pulmonary fibrosis. Asbestosis remains a significant clinical problem despite substantial reductions in occupational asbestos exposure, due to occupational exposure that occurred years earlier.
Clinical findings Most patients who develop asbestosis are asymptomatic for about 20 to 30 years after the initial exposure; the latency period between exposure and symptoms is inversely proportional to the intensity of asbestos exposure.
Symptoms The earliest symptom of asbestosis is usually the insidious onset of breathlessness with exertion. Dyspnea commonly progresses even in the absence of further asbestos exposure. Cough, sputum production, and wheezing are unusual; if present, these symptoms tend to be a consequence of cigarette smoking rather than asbestos- induced lung disease.
Physical examination As asbestosis progresses, patients may develop abnormal chest findings (bibasilar, fine end-inspiratory crackles) and clubbing; and Cor pulmonale (right sided heart failure) may ensue in advanced cases and may cause peripheral edema, jugular venous distension, hepatojugular refl ux.
Laboratory studies Laboratory studies are generally nonspecifi c and not useful clinically. Antinuclear antibodies, rheumatoid factor, and an elevated erythrocyte sedimentation rate may be present but do not correlate with disease severity or activity.
Evaluation The evaluation of suspected asbestosis in a patient with a history of asbestos exposure generally includes pulmonary function testing (spirometry) to assess the severity and pattern of lung impairment and imaging (Chest X-ray/ CT Chest) to look for characteristic features of asbestosis. Broncho alveolar lavage (BAL) has a limited role.
Diagnosis For the majority of patients, a confi dent clinical diagnosis of asbestosis can be made on the basis of the exposure history and the HRCT fi ndings. There are three key fi ndings that support the diagnosis of asbestosis: A reliable history of exposure to asbestos with a proper latency period from the onset of exposure to the time of presentation, and/ or presence of markers of exposure; Defi nite evidence of interstitial fi brosis, as manifested by one or more of the following: end-inspiratory crackles on chest examination; reduced lung volumes, presence of typical chest radiograph or HRCT fi ndings of interstitial lung disease, or histologic evidence of interstitial fi – brosis; and Absence of other causes of diffuse parenchymal lung disease.
Management There is currently no specific treatment for asbestosis. There have been no prospective studies of patients with asbestosis utilising anti-inflammatory or immunosuppressive agents, such as glucocorticoids or cytotoxic therapy, or antifibrotic agents. The absence of inflammation on histopathology examination makes it unlikely that anti-inflammatory or immunosuppressive agents would be of benefit. Thus, management of patients with asbestosis should focus on preventive and supportive measures, including: Smoking cessation;
Early detection of physiologic and radiographic abnormalities to aid prevention of further airborne asbestos exposure; Supplemental oxygen when there is resting hypoxemia or exercise-induced oxygen desaturation;
Prompt treatment of respiratory infections; and
Pneumococcal and influenza vaccination.
Complications Respiratory failure; and Malignancy. Malignancy — although some investigators have questioned the causal relationship between asbestosis and bronchogenic carcinoma, most studies have demonstrated a clear association between the two entities The risk of lung cancer associated with asbestos is greatly magnified by coexisting exposure to tobacco smoke.
Dr Romika Lata is a general practitioner at Oceania Hospitals Pte Ltd. The views expressed are the author’s and do not reflect the views of this newspaper.